
Billing Six-Figure Therapies
What to do when the charge exceeds Medicare claim limits.
Cell and gene therapies, such as CAR-T and the newly approved ENCELTO™ (revakinagene taroretcel-lwey), bring patients life-changing results, but also six-figure price tags that test the limits of the Medicare claims processing system. Providers often encounter claim rejections because the charge amount exceeds the maximum value these systems can process. The Centers for Medicare & Medicaid Services (CMS) and several Medicare Administrative Contractors (MACs) recently issued guidance on how to correctly report high-dollar charges.
Why High-Dollar Claims Reject
Medicare claims processing systems were built decades ago with fixed-length data fields. Each field that captures a charge amount is limited to seven digits, including the cents. As a result, the highest amount the system can accept is $99,999.99. Any dollar amount greater than that exceeds the numeric capacity of the field and cannot be stored or processed correctly. When a charge above that threshold is entered, the system generates a front-end rejection because the number will not fit into the field.
These rejections are not denials in the policy sense — they are technical system edits. The claim does not even enter the adjudication process. It is rejected immediately without being processed, typically returning with an edit or reason code indicating “invalid dollar amount.” There is no way to override or appeal this limitation because the rejection occurs at the system level rather than through a medical or policy review.
How to Correctly Bill High-Dollar Claims
Some providers mistakenly believe they can avoid the problem by rounding down the amount or submitting a paper claim, but neither option works. Rounding down or underreporting charges is a compliance risk because it misrepresents the true cost of the service and can distort cost reporting and reimbursement calculations. Paper claims also undergo electronic conversion and validation through the same systems, so the $99,999.99 limit still applies.
The only compliant way to bill amounts that exceed this system limitation is to split the line item or the claim into multiple parts. Each line or claim should remain under the $99,999.99 threshold, and the provider must document clearly in the remarks field that the split is due to CMS’ dollar field size limitation. This ensures the claim processes correctly, reflects the full and accurate charge, and prevents duplicate denials.
Understanding Fractional Billing
High-cost biologics and gene therapies may trigger not only the $99,999.99 charge limit but also fractional-unit billing requirements. To handle this, CMS created modifier LU — Fractionated payment.
Modifier LU applies only to specific therapies — most notably, certain CAR-T and other cell/gene therapies covered under national coverage determination (NCD) 110.24 — when the total allowed amount for one unit exceeds seven digits. The modifier tells the MAC that the claim lines represent fractional portions of one covered unit, not multiple separate services. Depending on payer policy, modifier 76 (Repeat procedure or service by same physician or other qualified health care professional) may also be necessary to identify subsequent fractional units on additional lines or claims.
Tip: Always follow MAC-specific fractionation guidance, as some may require 0.1-unit splits, others 0.25 or 0.5, etc.
Steps for Fractional Billing
When charges on a given line exceed the $99,999.99 limit for Medicare claims processing systems, the fix is to split the line or claim following MAC-specific guidance.
Step 1: Check payer billing policy
Some MACs (e.g., Palmetto GBA) instruct providers to file both lines on one claim; other MACs (e.g., Novitas Solutions) may require two separate claims. Always verify local MAC policy before claim submission.
Step 2: Split lines that exceed the dollar limit
Split the charge across two or more lines for the same date of service and code.
Use unequal dollar amounts and/or units (e.g., $99,999.99 and $22,000.01).
Include clear remarks such as “Line 1 of 2 – split due to CMS dollar limit” and “Line 2 of 2 – remaining amount.”
Apply modifier LU to each line/claim.
Apply modifier 76 to subsequent fractional units.
Confirm supporting documentation in the medical record.
Step 3: Apply JW/JZ correctly for single-use vials
Split billing does not remove your responsibility to report wastage accurately:
Use modifier JW for discarded amounts and modifier JZ if no wastage occurred.
Apply the modifiers on each split line as appropriate.
Examples of Fractional Billing
Always use unequal charges or units. Equal splits may trigger duplicate denials.
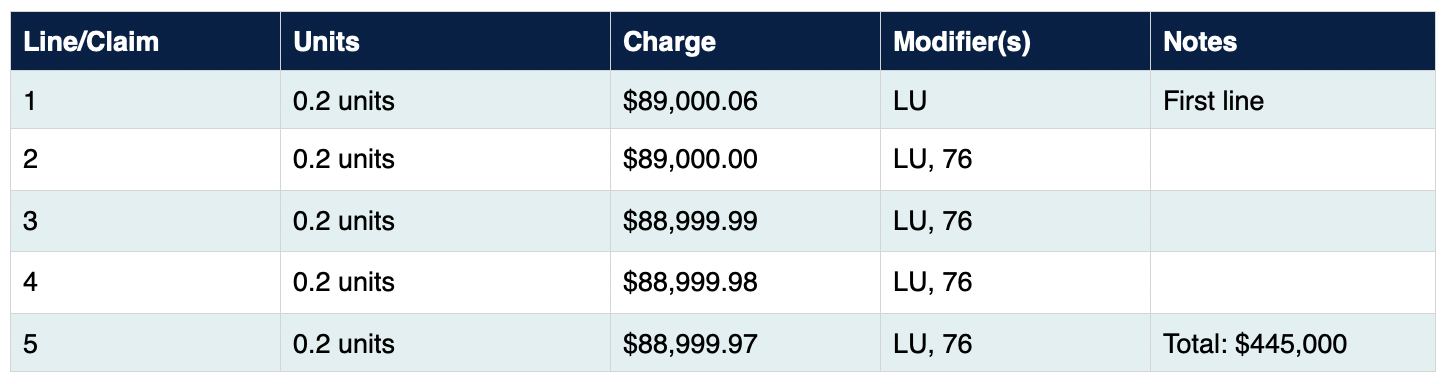
CAR-T Therapy
CAR-T services, governed under NCD 110.24, are among the most frequent high-dollar claims impacted by the field limit. CMS acknowledges in Transmittal R11774CP that these lines may need splitting.
Example: Charge per unit of CAR-T cell product is $445,000.
CAR-T Fractional Billing Example
ENCELTO™ (revakinagene taroretcel-lwey)
Beginning October 1, 2025, ENCELTO™ is billed under J3403 (per implant). Example: Charge per unit of ENCELTO™ implant is $250,000.
ENCELTO™ Fractional Billing Example

Key Takeaway
Proper structuring and claims submission practices keep lifesaving therapies like CAR-T and ENCELTO™ from being delayed by Medicare claims processing system edits and ensure providers receive full reimbursement in compliance with payer policy.
Resources
Novitas Solutions: Billing High-Cost Drugs and JW/JZ Modifier Requirements — https://www.novitas-solutions.com/webcenter/portal/MedicareJH/pagebyid?contentId=00142500
CGS: Submitting Claims When the Billed Amount Exceeds $99,999.99 — https://www.cgsmedicare.com/jc/pubs/news/2025/01/cope169968.html
Palmetto GBA, Jurisdiction J Part B: Submitting Claims for Amounts Greater Than $99,999.99 — https://dominoapps.palmettogba.com/palmetto/jjb.nsf/DIDC/PL2QB93VIM
Disclaimer: The coding guidance and regulatory requirements described in this article are provided for general informational purposes. Coding logic and reimbursement mechanics vary by payer and setting. Hospitals and manufacturers should consult with compliance, legal, and coding counsel prior to implementing changes.
